Carpal tunnel syndrome isn't just a sore wrist-it's a nerve compression that can steal your grip, your sleep, and your ability to do simple tasks like opening a jar or typing on a keyboard. It’s the most common nerve compression problem in the upper body, affecting about 1 in 10 people in the U.S., especially women and those between 45 and 60. If you’ve woken up with numb fingers, or found yourself shaking your hand like you’re trying to甩掉水珠, you’re not imagining it. This is real, and it gets worse if ignored.
What Exactly Is Happening in Your Wrist?
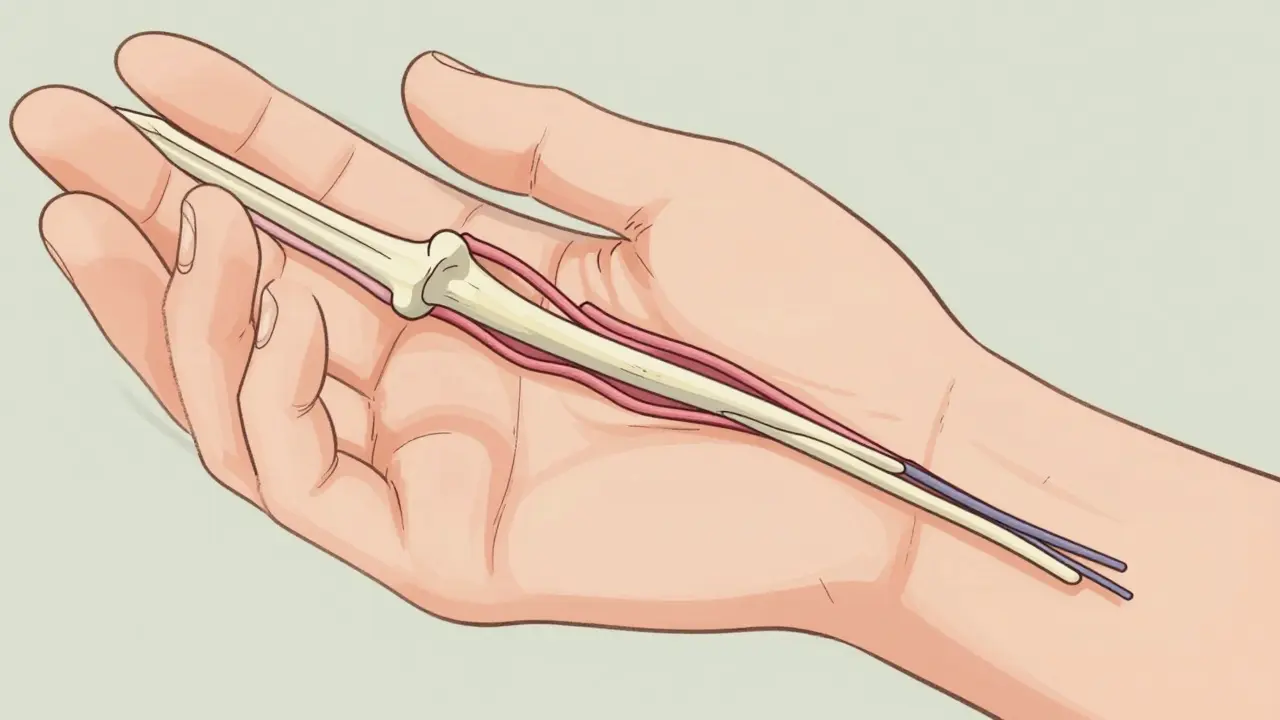
Your wrist isn’t just bone and skin. Inside it, there’s a narrow passageway called the carpal tunnel, formed by wrist bones on one side and a tough ligament on the other. Nine tendons that bend your fingers and thumb squeeze through it, along with the median nerve. That nerve controls sensation in your thumb, index, middle, and half of your ring finger. When that tunnel gets tight-because of swelling, repetitive motion, or even just anatomy-the nerve gets squished.It’s not just pressure. The compression cuts off blood flow to the nerve, causing swelling inside the nerve itself. Over time, the protective coating around the nerve fibers (myelin) starts to break down. If this goes on for months or years, the nerve fibers themselves can die. That’s when numbness turns permanent, and your thumb muscles begin to waste away.
How Do You Know It’s Carpal Tunnel-and Not Just a Cramp?
The symptoms don’t show up randomly. They follow a pattern:- Numbness or tingling in the thumb, index, middle, and part of the ring finger-never the pinky. That’s a key clue.
- Symptoms hit hardest at night. You wake up needing to shake your hand like it’s asleep.
- Daytime symptoms creep in: difficulty holding a coffee cup, fumbling buttons, dropping things.
- Pain can shoot up your forearm, sometimes all the way to your shoulder.
Doctors use simple tests to confirm it. The Phalen test-bending your wrists forward for a minute-triggers tingling if the nerve is compressed. The Tinel sign-tapping the inside of your wrist-makes a zap go down your fingers. The carpal compression test, where pressure is applied directly over the tunnel, often reproduces symptoms within 30 seconds.
For certainty, doctors may order nerve conduction studies. These measure how fast electrical signals move through the median nerve. If the signal slows down past 3.7 milliseconds across the wrist, it’s a clear sign of damage. But here’s the catch: about 15-20% of people over 60 show abnormal nerve tests even when they have no symptoms. That’s why diagnosis must always match what you’re feeling, not just what a machine says.
Three Stages of Carpal Tunnel-And Why Timing Matters
This isn’t a one-size-fits-all condition. It progresses in stages:- Mild: Symptoms come and go, mostly at night. You feel better after shaking your hand. This is the sweet spot for treatment.
- Moderate: Symptoms start during the day. You’re holding your wrist in weird positions to avoid the buzz. Simple tasks take more effort.
- Severe: Numbness is constant. Your thumb muscles look sunken. You can’t pick up a coin or turn a key. This is where damage becomes permanent.
Studies show that if you wait more than 12 months before treating it, conservative methods like splinting or injections only work about 35% of the time. If you act within 10 months, success jumps to 75%. That’s not a small difference-it’s the line between recovery and lifelong disability.
First-Line Treatments: What Actually Works
Before you think surgery, try what most doctors recommend first:- Wrist splints at night: This is the #1 recommended treatment. A splint keeps your wrist straight, preventing the tunnel from closing when you sleep. Studies show 60-70% of people with mild to moderate CTS get significant relief after 4-6 weeks of consistent use. Don’t just grab any splint-get one that holds your wrist at 0-10 degrees of extension. Too much bend or too much straightness won’t help.
- Activity changes: Avoid bending your wrist more than 30 degrees. That means adjusting your keyboard height, using voice-to-text, or switching from a mouse to a trackball. If you’re a cashier, a mechanic, or a nurse, your job might be part of the problem. Small changes add up.
- Nerve gliding exercises: These aren’t stretches. They’re gentle movements that help the median nerve slide through the tunnel without getting stuck. Do them 2-3 times a day. A physical therapist can show you the right way-do it wrong, and you’ll make it worse.
- Corticosteroid injections: These reduce swelling around the nerve. About 70% of patients get relief for 3 to 6 months. It’s not a cure, but it can buy you time to try other options. If you’ve had two injections and still feel the same, it’s time to think about surgery.
The cost of conservative care? Around $450-$750 in the U.S., including splints, therapy, and one injection. It’s a fraction of surgery-and if it works, you avoid the risks entirely.

Surgery: When It’s Time to Cut It Out
If your symptoms are severe, or if you’ve tried everything for 6-8 weeks with no improvement, surgery is the next step. The goal? Cut the ligament pressing on the nerve. Two main methods:- Open release: A 2-inch incision on the palm. The surgeon cuts the ligament directly. It’s reliable, well-studied, and cheaper.
- Endoscopic release: One or two tiny cuts. A camera guides a small tool to cut the ligament from inside. Recovery is faster, but it costs 15-20% more.
Both have a 90-95% success rate. That means most people regain normal sensation and strength. But it’s not perfect. About 15-30% of patients get “pillar pain”-tenderness on the sides of the palm that can last weeks or months. Scar tenderness happens in 5-10%. Nerve injury is rare-under 1%-but it can happen.
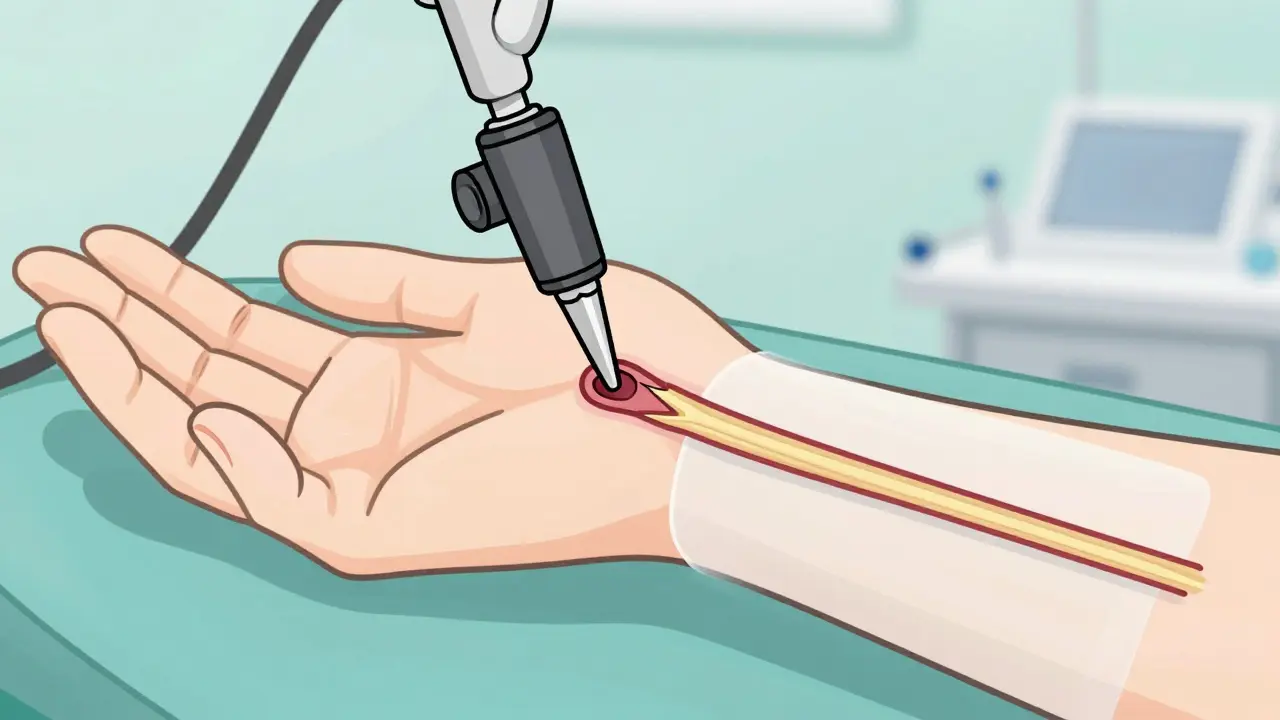
A newer option is ultrasound-guided percutaneous release, approved by the FDA in 2021. A tiny knife is inserted through the skin, guided by real-time ultrasound. It’s less invasive, causes 40% less pain, and patients return to work 50% faster. It’s not available everywhere yet, but it’s the future.
What Recovery Looks Like
After surgery, you’ll wear a bandage for a few days. Don’t lift heavy things for 2 weeks. Most people go back to light work in 2-3 weeks. Full recovery takes 6-8 weeks. If your job involves heavy lifting or repetitive motion, you might need 10-12 weeks before returning to full duty.Physical therapy after surgery isn’t optional-it’s essential. You’ll need 6-8 sessions to rebuild strength, reduce scar tissue, and retrain your hand. Skipping it increases your risk of stiffness and lingering pain.
Who’s Most at Risk-and Why
It’s not just computer users. The biggest risk groups are:- Healthcare workers: Nurses, orderlies, and dental hygienists-repetitive gripping and wrist flexion.
- Assembly line workers: Fast, repetitive motions with tools or parts.
- Food service workers: Chopping, slicing, and gripping knives and utensils.
Women are three times more likely to get it than men. Why? Smaller carpal tunnels. Pregnancy, menopause, and thyroid issues also raise risk because they cause fluid retention, which swells the tunnel.
And yes-your phone habits matter. Spending hours scrolling with your wrist bent? It won’t cause CTS alone, but it can push someone already on the edge over the line.
What Doesn’t Work (And Why You Should Skip It)
There’s a lot of noise out there:- Yoga or stretching alone: May help circulation, but won’t relieve nerve compression. Don’t delay real treatment.
- Acupuncture: Some people feel better temporarily, but no strong evidence it changes the nerve damage.
- Supplements (B6, magnesium): No reliable proof they help CTS. Don’t waste money.
- Waiting for it to “get better on its own”: This is the biggest mistake. Nerve damage is cumulative. Once it’s gone, it doesn’t come back.
Prevention Is Possible-Here’s How
You don’t have to wait for pain to start:- Keep your wrists neutral. Don’t rest them on hard edges while typing.
- Take breaks every 30 minutes. Stretch your fingers, shake your hands, roll your wrists.
- Use ergonomic tools: vertical mice, split keyboards, padded grips.
- Manage health conditions: Diabetes, arthritis, and thyroid disease increase risk. Keep them under control.
And if you’re in a high-risk job, talk to your employer. The U.S. has no federal CTS prevention rules, but the EU does. You deserve a workspace that doesn’t break your body.
What to Do Next
If you’re having symptoms:- Start wearing a wrist splint at night-right now.
- Track your symptoms: When do they happen? What makes them better or worse?
- See a doctor within 2 weeks. Don’t wait for it to get worse.
- Ask about nerve conduction studies if the diagnosis isn’t clear.
- Get physical therapy if recommended.
Carpal tunnel syndrome isn’t a life sentence. It’s a warning sign-and if you act early, you can stop it before it steals more than just your sleep.
Can carpal tunnel syndrome go away on its own?
Rarely. Mild symptoms might improve with rest or a splint, but the underlying nerve compression doesn’t fix itself. If you wait too long, the nerve damage becomes permanent. Early action is the only way to avoid long-term problems.
Is carpal tunnel surgery risky?
It’s one of the most common hand surgeries, with a 90-95% success rate. The biggest risks are temporary pillar pain (15-30% of cases) and scar tenderness. Nerve injury is rare-under 1%. For people with severe symptoms, the risk of not having surgery is much higher than the risk of having it.
Do I need an MRI or X-ray to diagnose carpal tunnel?
No. X-rays and MRIs don’t show nerve compression well. The gold standard is nerve conduction studies. Ultrasound is also becoming common-it can measure the size of the median nerve and show swelling. Most diagnoses are made with physical exams and these tests, not imaging.
Can typing cause carpal tunnel syndrome?
Typing alone rarely causes CTS. But if you already have a narrow carpal tunnel, or you’re bending your wrist while typing for hours, it can trigger symptoms. It’s not the typing-it’s the wrist position. Using a neutral wrist posture and taking breaks reduces risk.
How long does it take to recover from carpal tunnel surgery?
Most people return to light work in 2-3 weeks. Full recovery takes 6-8 weeks. If your job involves heavy lifting or repetitive motion, you may need 10-12 weeks. Physical therapy helps speed up recovery and prevents stiffness.
Are wrist splints really effective?
Yes-for mild to moderate cases. Studies show 60-70% of people get significant relief using a splint at night, especially if worn consistently for 4-6 weeks. It’s the first-line treatment because it’s low-risk and low-cost. But it won’t help if the nerve is already severely damaged.
Can carpal tunnel come back after surgery?
It’s uncommon, but possible. If the ligament regrows or scar tissue forms around the nerve, symptoms can return. This happens in fewer than 5% of cases. Maintaining good wrist posture and avoiding repetitive strain helps prevent recurrence.
Is carpal tunnel syndrome genetic?
Not directly, but your anatomy is. If you have a naturally narrow carpal tunnel, you’re more likely to develop it. This trait can run in families. Women, especially those with smaller wrists, are more prone. So while it’s not inherited like a disease, your body’s structure plays a big role.










January 25, 2026 AT 04:35
I’ve been wearing a splint at night for six weeks now. Honestly? Game changer. Used to wake up with my hand screaming, now I just roll over and go back to sleep. No magic cure, but it’s the only thing that didn’t make me want to chuck my keyboard out the window.
Also, the nerve gliding exercises? Took me a week to stop doing them wrong. YouTube helped. Don’t just wing it.