
Inflammation is a protective immune response that involves blood vessels, immune cells, and molecular messengers. In the lungs, this response becomes the engine behind many asthma attacks.
Asthma isn’t just wheezing; it’s a chronic condition where the airways overreact to triggers. Understanding why that over‑reaction happens means digging into the inflammatory cascade that narrows and tightens the bronchi.
What asthma really is
Asthma is a chronic respiratory disease marked by airway hyperresponsiveness, inflammation, and reversible bronchoconstriction. When a person inhales an allergen, cold air, or pollutants, the already‑sensitized airway walls swell, produce excess mucus, and the smooth muscle tightens. The result: coughing, shortness of breath, and that familiar chest tightness.
Two key players dictate the type of inflammation: Eosinophils are a type of white blood cell that releases toxic proteins and lipids during allergic reactions. The other is Neutrophils, which respond quickly to bacterial infections and produce enzymes that can damage tissue.
How inflammation starts in the airway
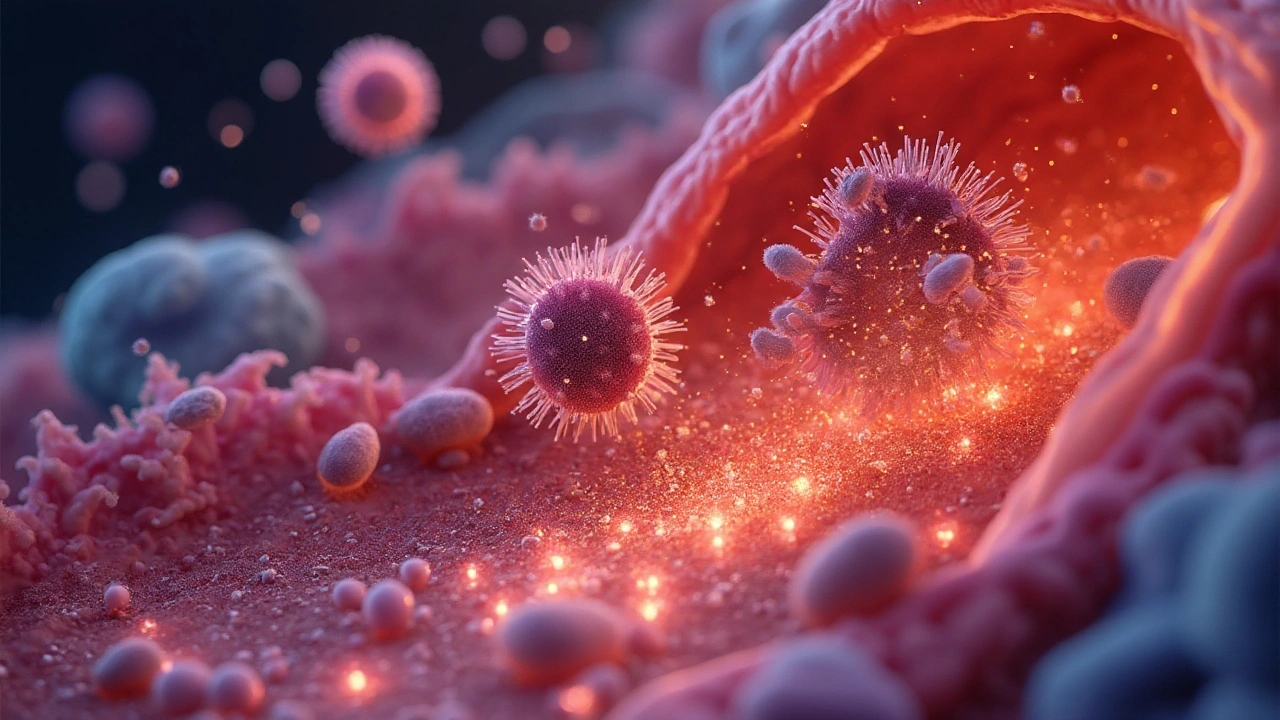
Every inflammatory episode begins with an environmental trigger such as pollen, smoke, or viral infection. The airway epithelium releases alarm signals-called cytokines-that call immune cells to the scene. Common cytokines in asthma include interleukin‑4 (IL‑4), IL‑5, and IL‑13. These molecules not only recruit eosinophils but also stimulate the production of IgE antibodies, which sensitize mast cells for future attacks.
Once eosinophils settle in the airway wall, they degranulate, spilling major basic protein, eosinophil peroxidase, and other cytotoxins. The toxins damage the epithelium, turning a smooth lining into a ragged barrier that leaks fluids, inviting more immune cells. This self‑perpetuating loop is why a single trigger can spiral into a full‑blown asthma exacerbation.
Cellular profiles: eosinophilic vs neutrophilic asthma
| Feature | Eosinophilic asthma | Neutrophilic asthma |
|---|---|---|
| Predominant cell | Eosinophils | Neutrophils |
| Typical biomarkers | Blood eosinophil count >150cells/µL, FeNO ↑ | sputum neutrophils >60%, IL‑8 ↑ |
| Response to inhaled corticosteroids | Good to excellent | Poor - often steroid‑resistant |
| Common triggers | Allergens, seasonal pollen | Smoking, bacterial infection, occupational dust |
| Targeted biologic therapies | Anti‑IL‑5 (e.g., mepolizumab) | Anti‑IL‑17 or anti‑CXCR2 under trial |
The table shows why a one‑size‑fits‑all approach rarely works. Identifying the cellular phenotype guides treatment, especially when standard inhaled corticosteroids fail to curb symptoms.
Treatment rooted in inflammation control
Traditional corticosteroid therapy works by dampening cytokine production, reducing eosinophil survival, and tightening the leaky airway barrier. However, not everyone tolerates high‑dose inhaled steroids, and long‑term use can lead to oral thrush, hoarseness, and bone loss.
This is where biologic therapy steps in. Biologics are engineered antibodies that lock specific cytokines or cell receptors, effectively neutralising the inflammatory signal. For eosinophilic asthma, anti‑IL‑5 drugs (mepolizumab, reslizumab, benralizumab) slash exacerbation rates by up to 50%.
For patients with neutrophilic, steroid‑resistant disease, the pipeline includes anti‑IL‑17 (secukinumab) and anti‑CXCR2 agents that block neutrophil trafficking. While still under investigation, early data show promise in reducing emergency visits.
Practical steps to tame airway inflammation
- Track triggers: Keep a diary of symptoms, pollen counts, and exposure to smoke or chemicals.
- Check biomarkers: Blood eosinophil counts and fractional exhaled nitric oxide (FeNO) help decide if steroids or biologics are appropriate.
- Adhere to controller meds: Even on a biologic, inhaled corticosteroids remain the backbone for most patients.
- Vaccinate: Influenza and COVID‑19 vaccines lower the risk of viral‑induced exacerbations.
- Stay active: Regular aerobic exercise improves lung capacity and reduces overall inflammation.
These habits, coupled with personalized medication, create a two‑pronged defense: prevent the inflammatory spark and blunt its downstream effects.
Future directions - what’s on the horizon?
Scientists are mapping the “asthma exposome”, a comprehensive picture of all environmental and lifestyle factors that drive inflammation. Wearable air‑quality sensors, integrated with mobile apps, could alert patients the moment they step into a high‑pollution zone, prompting pre‑emptive inhaler use.
On the molecular side, single‑cell RNA sequencing is revealing sub‑populations of airway immune cells that respond differently to the same cytokine cocktail. This may lead to ultra‑targeted therapies that silence only the harmful pathways while preserving protective immunity.
Finally, epigenetic research suggests that early‑life exposure to certain microbes can re‑program airway immune cells, potentially preventing asthma from developing in the first place. While still experimental, these insights hint at a future where we treat the root cause-dysregulated inflammation-rather than just the symptoms.
Putting it all together
The link between inflammation and asthma is a classic cause‑and‑effect story. Environmental triggers set off cytokine storms, which recruit eosinophils or neutrophils, leading to airway narrowing and the classic wheeze. By decoding the cellular and molecular players, clinicians can match patients with the right anti‑inflammatory strategy-whether that’s a low‑dose inhaler, an anti‑IL‑5 biologic, or a future epigenetic intervention.
When you understand the "why" behind each flare‑up, you gain the power to stop it before it starts.
Frequently Asked Questions
What exactly triggers airway inflammation in asthma?
Common triggers include allergens (pollen, dust mites), viral infections, tobacco smoke, cold air, and occupational chemicals. Each trigger prompts airway epithelial cells to release cytokines like IL‑4, IL‑5, and IL‑13, which recruit inflammatory cells and set off the cascade.
How do doctors determine if I have eosinophilic or neutrophilic asthma?
Physicians measure blood eosinophil counts, FeNO levels, and sputum cell differentials. High eosinophils (>150cells/µL) and elevated FeNO point to eosinophilic disease, while a sputum sample dominated by neutrophils (>60%) signals neutrophilic asthma.
Are inhaled corticosteroids enough for everyone?
Inhaled steroids are the first‑line controller for most asthma patients, but they work best when eosinophils drive the inflammation. People with neutrophilic, steroid‑resistant disease often need additional treatments like long‑acting bronchodilators or biologic agents.
What are the most effective biologic therapies right now?
For eosinophilic asthma, anti‑IL‑5 drugs (mepolizumab, reslizumab, benralizumab) have the strongest evidence, cutting severe exacerbations by about half. Anti‑IgE (omalizumab) works for allergic asthma. Emerging anti‑IL‑4Rα (dupilumab) helps both eosinophilic and allergic phenotypes.
Can lifestyle changes really reduce airway inflammation?
Yes. Regular aerobic exercise, a diet rich in omega‑3 fatty acids, quitting smoking, and maintaining a healthy weight all lower systemic inflammation and can improve lung function over time.
What should I do during an acute asthma flare?
Use your quick‑relief inhaler (usually a short‑acting beta‑agonist) immediately, sit upright, and practice slow breathing. If symptoms don’t improve within 5‑10 minutes, follow your action plan-often a repeat dose or a systemic steroid-and seek medical help if needed.






















September 24, 2025 AT 20:44
Inflammation is the spark, so keep your inhaler handy and avoid known triggers.