Imagine a medication that doesn't just lower your blood sugar, but actually changes how your brain feels about food. For years, managing type 2 diabetes meant balancing insulin and glucose without gaining weight-a difficult feat since many traditional diabetes drugs actually make you heavier. That changed with the rise of GLP-1 receptor agonists is a class of medications that mimic the glucagon-like peptide-1 hormone to improve insulin secretion and suppress appetite.
If you've heard of Ozempic, Wegovy, or Mounjaro, you're talking about these drugs. They have shifted the conversation from simply "managing" diabetes to actively reversing the metabolic markers of obesity. But how do they actually work inside your body to drop your A1C and your waistline simultaneously?
The Science of How GLP-1s Work
To understand these drugs, you first have to understand the hormone they mimic. Naturally, your body releases GLP-1 from the L-cells in your small intestine after you eat. It's like a signal to your body saying, "Food is here; get the metabolism ready."
When you take a GLP-1 receptor agonist, the drug activates receptors in two primary areas: the pancreas and the brain. In the pancreas, it stimulates beta cells to release insulin but only when your blood sugar is actually high. At the same time, it tells the alpha cells to stop releasing glucagon, the hormone that raises blood sugar. This dual action keeps your glucose levels stable without the "crash" often seen with older medications.
Then there is the gut factor. These medications slow down gastric emptying-essentially making your stomach empty into the small intestine 15-30% slower in the first hour after a meal. This prevents the massive blood sugar spikes that typically happen after a high-carb dinner, which is a huge part of why your A1C drops.
Why the Weight Loss is So Dramatic
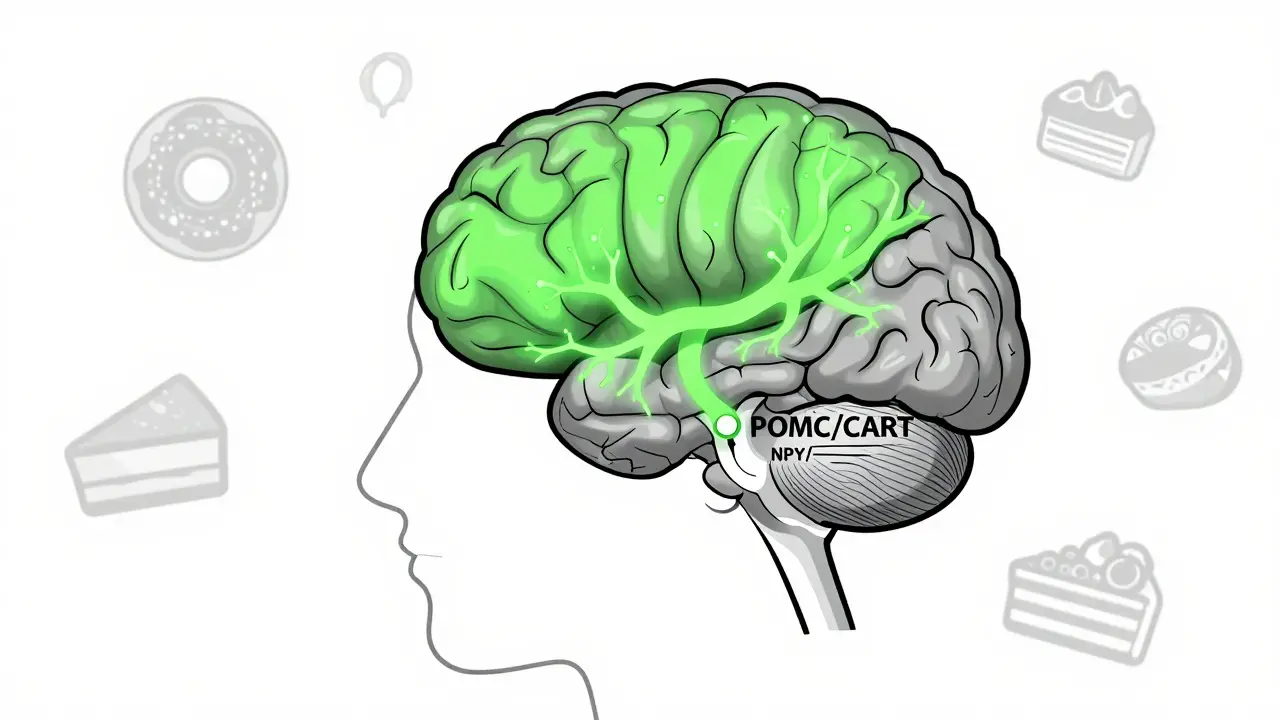
While the glucose control is great, the weight loss is what made these drugs famous. This happens because the drugs cross the blood-brain barrier and hit the hypothalamus, the area of the brain that controls hunger.
Specifically, they stimulate POMC/CART neurons (which tell you that you're full) and shut down NPY and AgRP neurons (which tell you that you're starving). This creates a "mindset shift." Many people describe it as "food noise" disappearing-the constant mental chatter about the next snack or a craving for sugar simply vanishes. Clinical data shows this can reduce appetite and hunger by as much as 30-40%.
The results are concrete. In the STEP 3 clinical trial, people using semaglutide (at a 2.4 mg weekly dose) lost an average of 15.3 kg (about 14.9% of their body weight) over 68 weeks. This is a level of weight loss that, until recently, was usually only possible through bariatric surgery.
Comparing GLP-1s to Other Diabetes Meds
If you're choosing a treatment plan, it's helpful to see how these stack up against the old guard. Most traditional diabetes drugs are "weight neutral" at best or "weight positive" at worst.
| Medication Class | A1C Impact | Weight Effect | Primary Mechanism |
|---|---|---|---|
| GLP-1 Receptor Agonists | High (1.0-1.8% reduction) | Significant Loss | Satiety + Insulin secretion |
| SGLT2 Inhibitors | Moderate | Mild Loss (2-5 kg) | Glucose excretion via urine |
| DPP-4 Inhibitors | Low (0.5-1.0% reduction) | Neutral | Slows GLP-1 breakdown |
| Sulfonylureas | High | Weight Gain | Forced insulin release |
| Insulin | Very High | Significant Gain | Direct glucose lowering |
As the table shows, GLP-1s are unique because they solve two problems at once. While SGLT2 inhibitors also help with weight, they do it by flushing sugar out through your kidneys, whereas GLP-1s change your appetite and metabolic rate.
The Different Versions: Ozempic, Wegovy, and Beyond
You'll notice different brand names for the same active ingredients. This is usually because the FDA approves different doses and labels for either "diabetes" or "weight loss."
- Semaglutide: Available as Ozempic (for diabetes) and Wegovy (for obesity). It is currently one of the most potent options for both A1C and weight.
- Liraglutide: Available as Victoza and Saxenda. This requires a daily injection rather than a weekly one, making it slightly less convenient.
- Dulaglutide: Sold as Trulicity, known for a very easy-to-use once-weekly pen.
- Tirzepatide: Sold as Mounjaro and Zepbound. This is a "dual agonist," meaning it mimics both GLP-1 and GIP hormones. In the SURMOUNT-1 trial, it showed an average weight loss of 20.2% at the highest dose-even beating semaglutide.

Managing the "Adjustment Period"
It's not all smooth sailing. Because these drugs slow down your digestion, your gut needs time to adapt. Between 30% and 50% of users experience gastrointestinal side effects. Nausea is the big one, affecting about 15-20% of patients, while some deal with vomiting or diarrhea.
The secret to avoiding these issues is slow titration. You don't just start at the full dose. For example, with Wegovy, you typically start at 0.25 mg for four weeks, then move to 0.5 mg, and so on, over about four months. If you jump too fast, your stomach won't keep up, and you'll likely spend your week feeling sick.
Pro tip: Many users find that taking the injection right before bed helps them "sleep through" the worst of the nausea. Avoiding high-fat, greasy meals during the dose-escalation phase also makes a world of difference, as fats stay in the stomach longer and can trigger nausea.
The Long-Term Reality: What Happens When You Stop?
Here is the part that doesn't always make the headlines: these are generally long-term medications. Data suggests that after stopping treatment, people regain an average of 50-70% of their lost weight within a year. This isn't because the drug "failed," but because the biological signals (the hunger and the slowed digestion) return to their original state.
However, the benefits extend beyond the scale. The LEADER trial showed that liraglutide reduced major adverse cardiovascular events by 13% in high-risk patients. We are also seeing promising data for non-alcoholic fatty liver disease and even heart failure with preserved ejection fraction.
Do I have to take GLP-1 injections forever?
For many, yes. Because these drugs manage a chronic biological condition (insulin resistance and appetite regulation), stopping them often leads to a return of hunger and a rise in A1C. However, some doctors use them as a "jumpstart" to establish healthy eating habits before tapering off.
Which is better: Ozempic or Mounjaro?
Mounjaro (Tirzepatide) is generally more potent because it targets two hormones (GLP-1 and GIP) instead of just one. Clinical trials show it typically results in greater weight loss and slightly stronger A1C reduction. That said, Ozempic has a longer track record of safety data.
Can I take these if I don't have diabetes?
Yes, specifically through versions like Wegovy or Zepbound, which are FDA-approved for chronic weight management in adults with a BMI of 30 or more, or 27 if they have a weight-related condition like hypertension.
How do I deal with the nausea?
Stick strictly to the titration schedule and avoid high-fat foods. Eat smaller, more frequent meals and stay hydrated. If nausea is severe, talk to your doctor about using over-the-counter options like dimenhydrinate.
Are there oral versions of these drugs?
Yes, there are oral formulations of semaglutide available in some markets (like Rybelsus). While more convenient than an injection, they often have stricter administration rules, such as taking them on an empty stomach with a small sip of water.




April 4, 2026 AT 04:11
The point about food noise is the real game changer here. Most people don't realize that hunger isn't just about a rumbling stomach, it's a mental obsession that makes willpower almost irrelevant for some. If you're starting out, definitely prioritize protein and electrolytes since you'll be eating way less and can hit a wall pretty quickly.