When your liver can't do its job, your brain starts to pay the price. Hepatic encephalopathy (HE) isn't a disease you can see on an X-ray. It's a quiet, creeping change in how your mind works-confusion, forgetfulness, slurred speech, even coma-caused by one thing: too much ammonia in your blood. And for people with advanced liver disease, this isn't rare. About 4 in 10 cirrhosis patients will develop overt HE at some point. The good news? It’s often reversible. The better news? We know exactly how to stop it before it starts.
What Exactly Is Hepatic Encephalopathy?
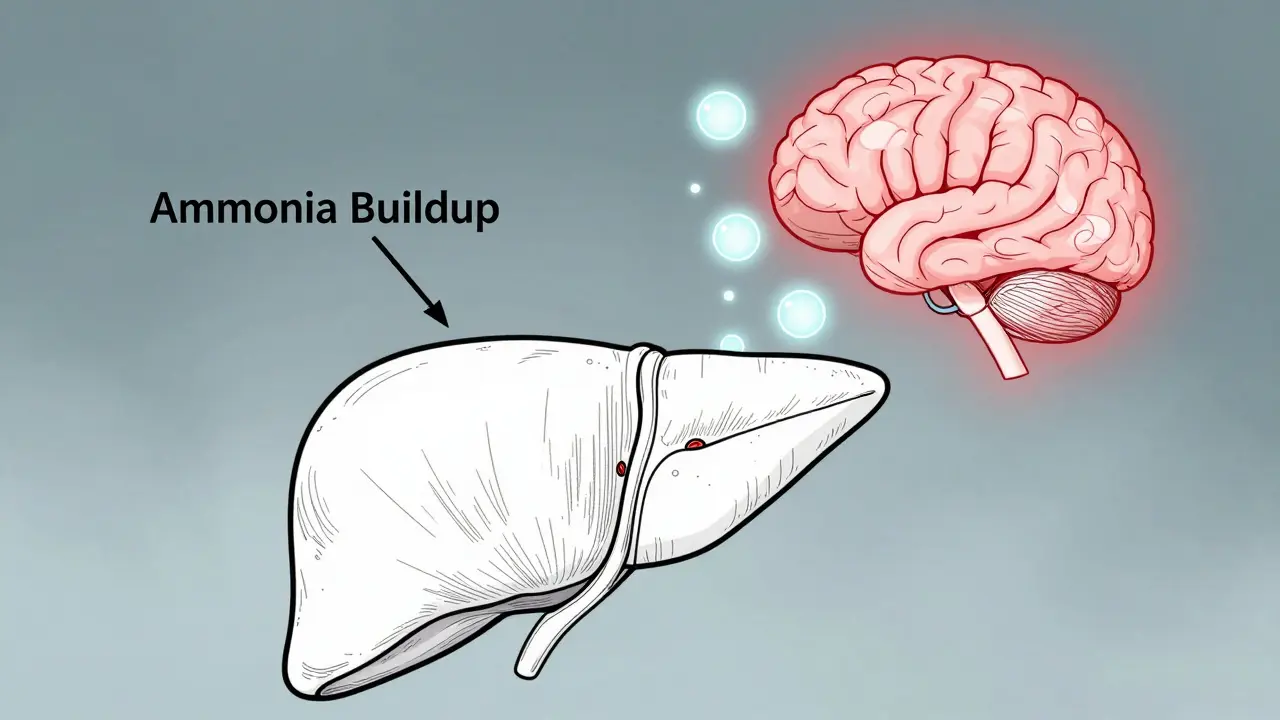
Hepatic encephalopathy happens when your liver fails to filter out toxins, especially ammonia. Normally, your liver breaks down ammonia, a waste product from protein digestion, into harmless urea. But when scar tissue from cirrhosis blocks blood flow, ammonia slips through untouched. It enters your bloodstream, crosses the blood-brain barrier, and starts messing with brain cells. The result? A spectrum of neurological symptoms that can sneak up slowly or hit hard and fast.
There are three types. Type A shows up suddenly with acute liver failure-often from drug overdoses like acetaminophen. Type B happens when blood bypasses the liver entirely due to abnormal shunts, even if the liver itself is still healthy. But Type C? That’s the most common. It’s the one tied to chronic liver disease, especially cirrhosis. And it’s the one we can prevent.
Symptoms don’t appear out of nowhere. They follow a pattern. Grade 1 might just be trouble sleeping or mild forgetfulness. Grade 2? Personality shifts, irritability, trouble doing simple math. By Grade 3, speech becomes slurred, confusion deepens. Grade 4 is coma. But here’s the thing: many people have minimal HE long before anyone notices. That’s when cognitive tests show subtle brain slowdowns-slower reaction times, poor attention-yet the person feels fine. Left unchecked, minimal HE often turns into overt HE.
Why Lactulose Is the Cornerstone of Treatment
Since the 1960s, lactulose has been the go-to drug for HE. It’s not a miracle cure. But it’s reliable, cheap, and works directly on the root cause: gut ammonia.
Lactulose is a synthetic sugar your body can’t digest. When it reaches your colon, bacteria break it down into acids. That drops the pH in your gut from neutral (7) to acidic (5-6). Ammonia (NH₃) in that environment turns into ammonium (NH₄⁺). And ammonium? It can’t cross into your bloodstream. It gets trapped and flushed out with your stool.
The goal? Two to three soft bowel movements a day. Not more, not less. Too few, and ammonia builds up. Too many, and you’re dehydrated, dizzy, or too weak to function. Dosing is personal. Most start with 30-45 mL, taken three to four times daily. Some need more. Others get by with less. The key? Adjust until you hit that sweet spot.
Here’s what patients say: 79% deal with diarrhea. 62% get cramps. 54% hate the taste-it’s sweet, syrupy, and leaves a weird aftertaste. One man on Reddit shared, “Lactulose saved me from hospitalization, but the constant bathroom trips ruined my job interviews.” That’s real. But for many, the trade-off is worth it. A patient on Hep Forums reported, “After six months of lactulose and rifaximin, my cognitive scores improved. I went back to part-time work.”
But here’s the catch: 65% of people who don’t respond to lactulose aren’t taking enough. A 2023 University of Michigan study found most non-responders were on less than 30 mL per day. That’s not enough. Doctors often underdose out of fear of side effects. But the data says: push for the right stool frequency. It’s not about discomfort-it’s about saving your brain.
When Lactulose Isn’t Enough: Rifaximin and Other Options
For people with recurrent HE, lactulose alone isn’t always enough. That’s where rifaximin comes in.
Rifaximin (brand name Xifaxan) is an antibiotic that doesn’t get absorbed into your bloodstream. It stays in your gut and kills ammonia-producing bacteria like Klebsiella and Proteus. Since its FDA approval in 2010, it’s cut recurrent HE episodes by 58% compared to placebo. The standard dose? 550 mg twice daily. It’s expensive-around $1,200 a month-but when combined with lactulose, it’s often life-changing.
There are alternatives. L-ornithine-L-aspartate (LOLA) helps your liver process ammonia through natural pathways. Studies show it improves mental status by 35%. But it’s not widely available everywhere. And then there are the emerging options. SYN-004, a gut-targeted antibiotic, reduced HE episodes by 35% in recent trials. Fecal microbiota transplants (FMT) have normalized ammonia in 70% of refractory cases. And in Japan, AST-120-an oral adsorbent that binds toxins in the gut-has been used since 2005 and is now approved in Europe.
But here’s the reality: most people still get treated with lactulose and rifaximin. Why? Because they work. And because alternatives are still experimental or hard to access.
Prevention Is the Best Medicine
Preventing HE is easier than treating it. And it starts with three things: avoiding triggers, managing protein, and staying ahead of symptoms.
First, identify what sets off your episodes. Spontaneous bacterial peritonitis? That’s 25-30% of cases. Upper GI bleeding? Another 20-25%. Electrolyte imbalances-especially low potassium-cause 15-20%. One caregiver on Reddit tracked her husband’s flares for months and found: urinary tract infections always preceded his confusion. Now she tests monthly. Result? 80% fewer episodes.
Second, don’t cut protein long-term. You might think, “Less protein = less ammonia.” But your body needs protein to maintain muscle, fight infection, and heal. The guidelines say: during an acute HE episode, limit protein to 0.5 g per kg of body weight. Once you recover, go back to 1.2-1.5 g/kg. That’s about 70-90 grams a day for most adults. Think eggs, lean meat, tofu, lentils. Don’t fear protein-just don’t overdo it.
Third, avoid sedatives. Benzodiazepines (like Valium or Xanax) can worsen HE by 3.2 times. Even occasional use is risky. Sleep aids? Talk to your doctor. Over-the-counter antacids? Some contain aluminum-avoid them. And never skip your lactulose, even if you feel fine. A 2022 study found that patients who took prophylactic lactulose (15 mL twice daily) cut their HE recurrence by half in just six months.
Why Ammonia Levels Don’t Always Tell the Whole Story
Doctors used to rely on blood ammonia tests. High ammonia? Must be HE. Low ammonia? You’re fine.
That thinking is outdated. Research now shows ammonia levels don’t reliably match symptoms in chronic liver disease. A 2021 study by Dr. Jasmohan Bajaj found that some patients with severe confusion had normal ammonia. Others with high ammonia showed no symptoms at all. So why test it?
It’s not useless. In acute liver failure, ammonia trends can guide treatment. But for cirrhosis patients? Focus on symptoms, not numbers. If you’re confused, forgetful, or acting out of character-treat it as HE. Don’t wait for a lab result.
That’s why tools like the EncephalApp Stroop test are gaining traction. It’s a free mobile app that takes 5 minutes. It measures attention and processing speed. If your score drops, it’s an early warning. Family members often spot changes 48-72 hours before doctors do. Keep a journal. Note mood swings, sleep changes, trouble concentrating. These are your early flags.

What Happens If It’s Ignored?
Left untreated, HE doesn’t just fade away. It progresses. Each episode leaves behind subtle brain damage. Memory gets worse. Reaction times slow. Your ability to work, drive, or live independently declines.
Severe HE can lead to coma. About 15-20% of acute HE cases require ICU admission for airway protection. Mortality in those cases? 25-30%. And the cost? A single hospitalization for acute HE runs $28,500. Outpatient management? Just $1,200. Prevention isn’t just about health-it’s about money, independence, and dignity.
One of the biggest hidden dangers? Misdiagnosis. Nearly a third of HE patients are initially told they have dementia. The symptoms overlap: confusion, memory loss, personality changes. But HE is treatable. Dementia isn’t. If you have liver disease and notice mental changes, demand a liver evaluation. Don’t accept “it’s just aging.”
Final Thoughts: Small Steps, Big Impact
Hepatic encephalopathy is not a death sentence. It’s a signal. Your body is telling you your liver is struggling. And we have the tools to respond.
Take your lactulose. Hit your target stools. Watch for triggers. Keep protein in check. Avoid sedatives. Track your symptoms. Involve your family. If you’ve had HE before, ask about prophylactic dosing. If you’re on rifaximin, don’t stop without talking to your doctor.
For many, HE is a chronic condition. But with consistent management, it doesn’t have to control your life. People are returning to work. Driving again. Playing with grandchildren. All because they stuck with the basics.
The science is clear. The treatment works. The choice? It’s yours.
Can hepatic encephalopathy be reversed?
Yes, in most cases. Especially if caught early. Overt hepatic encephalopathy often improves or fully resolves with treatment like lactulose and rifaximin. Minimal HE can also improve with proper management. The key is addressing the underlying cause-usually high ammonia-and removing triggers like infections or constipation. However, repeated episodes can cause lasting cognitive changes, so prevention is better than cure.
How long does it take for lactulose to work?
Most people see improvement within 24 to 48 hours. The goal isn’t just symptom relief-it’s achieving two to three soft stools per day. If you haven’t had a bowel movement after 48 hours on a full dose, your dose may be too low, or there’s another trigger (like an infection or dehydration) that needs attention. Don’t wait. Call your doctor.
Is lactulose safe for long-term use?
Yes. Lactulose has been used safely for decades. It’s not absorbed into the bloodstream, so it doesn’t affect other organs. The main concerns are side effects like bloating, cramps, and diarrhea. These can be managed by adjusting the dose. Long-term use doesn’t lead to dependence or loss of effectiveness. The bigger risk? Stopping it too soon.
Can I drink alcohol if I have hepatic encephalopathy?
No. Alcohol is toxic to the liver and worsens liver damage, making HE more likely and harder to treat. Even small amounts can trigger a flare-up. If you have cirrhosis or a history of HE, complete alcohol abstinence is non-negotiable. It’s not about moderation-it’s about survival.
What foods should I avoid with hepatic encephalopathy?
Avoid high-sodium foods (salted meats, canned soups, chips) because they can cause fluid retention and worsen ascites. Limit processed foods with added sugars and unhealthy fats, which can worsen fatty liver. Avoid raw shellfish (risk of infection). During an acute episode, reduce protein temporarily-but don’t eliminate it long-term. Focus on plant-based proteins (lentils, tofu) and lean animal proteins (chicken, fish). Always consult a dietitian familiar with liver disease.
Are there any new treatments on the horizon?
Yes. Researchers are exploring several promising options. SYN-004 (ribaxamase) is a gut-targeted antibiotic that reduces ammonia-producing bacteria without systemic effects. Fecal microbiota transplants (FMT) are showing success in refractory cases. AST-120, an oral adsorbent already used in Japan, is gaining traction in Europe. And a new fixed-dose combo of lactulose and rifaximin (Xifaxilac) was approved in 2023. Long-term, the focus is shifting toward precision medicine-using blood biomarkers and smartphone-based cognitive monitoring to predict and prevent HE before symptoms appear.




